“Fear remains the most difficult barrier to overcome”
Margaret Chan WHO Director General
Recent headlines immediately drew my attention. Dispatches from Monrovia, the Liberian capital, reported that under presidential orders, armed riot police and soldiers from the Ebola Task Force in riot gear and equipped with automatic weapons had quarantined West Point, a northern township of the city, on August 20, 2014. To physically cordon off the district, makeshift barricades were erected using red rope lines, wood scraps, and barbed wire. Ferry service to the peninsula was cancelled and the coast guard started patrolling the surrounding waters, turning back people attempting to flee in their canoes. A subsequent image depicted a quarantine violator, summarily detained under the chassis of a car.
Segregation and detention of people suspected or suffering from lethal contagious diseases has a long past. In an era of globalization, “contagious anxieties” become ubiquitous. Responses towards an ever-more complex sequence of biological dangers tend to flourish especially in overcrowded urban settings like Monrovia. In despair, the lessons of history are conveniently ignored. Blaming the victim continues to be a common survival skill, employed for self-defense and preservation. Appealing to basic human instincts of survival, successive Western societies developed regulations and erected institutions designed to cope with incoming diseases. Like in Monrovia today, much was judged to be at stake: catastrophic mass dying, social breakdown, political chaos, economic decline, and, at times, even national survival.
Since the Renaissance, the term quarantine came to designate spaces for the temporary detentions of residents, travellers, and cargo suspected of carrying infection. This tactic differs somewhat from another traditional public health scheme: the sanitary cordon or blockade that closes checkpoints, roads, and borders with the similar purpose of preventing the spread and contamination of deadly infectious diseases. In both cases, groups of individuals previously marginalized on the basis of age, sex, race, religion, and class were blamed for epidemic outbreaks. The favorite scapegoats are often strangers, newcomers, and ethnic minorities. I am particularly sensitive to issues of stigma and isolation because of my recent research and completion of a book manuscript on the San Francisco Pesthouse, now under academic review. My thesis is that both fear and disgust historically managed to frame coping behaviors and drive actions. In my opinion, anger and revulsion explain the heartless, even brutal nature of the responses.
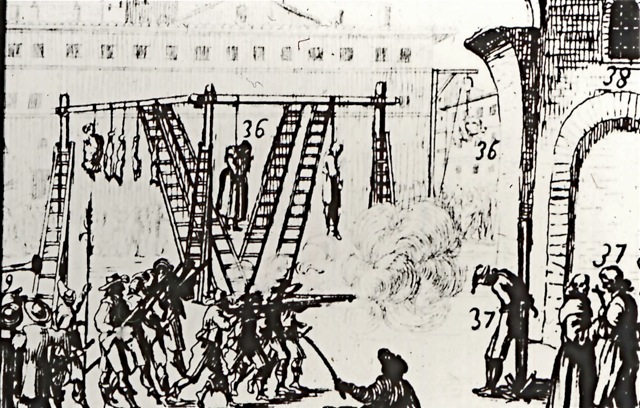
Plague in Rome 1665
In Liberia, Monrovia’s crowded and dilapidated slum with its narrow alleys and rickety shanties had long been a public health nightmare: neglected by authorities, residents were without sewage disposal and only obtained their water in wheelbarrows. Ebola was only the last and perhaps the most dangerous disease to visit this community of an estimated 75,000 people. With hospitals closing to prevent further institutional contamination—some health workers were already dead or dying, potential victims had not place to go. Without consulting residents, the government decided to use a former schoolhouse in West Point as a makeshift neighborhood center for the purpose of concentrating, isolating, and managing all Ebola cases reported in the city. This decision only stoked the growing local panic, leading to protests and violence. Perhaps Ebola was only a “government hoax.” The building was stoned and its patients—presumed to be infectious-- forced to flee. The attack led to widespread looting of furnishings and medical equipment, including blood-soaked bedding believed to be contagious.
Enforced by police and even military units, indiscriminate segregations often prove counterproductive: historically they fostered mistrust, fear and panic, resistance and aggression, while encouraging flight, concealment, and social chaos. Paradoxically, while often unsuccessful in curbing an epidemic, such containment policies contribute to the suffering and risk additional fatalities. Since the Black Death, families and isolated populations trapped in their homes and neighborhoods suffered severe hardships ranging from a lack of water, food supplies, and a higher risk of cross infection. Loss of employment and economic ruin followed. When an outbreak of plague in Rome occurred in 1656, the entire city was immediately closed with temporary stockades placed in front of two gates for screening supplies and people. Police patrols enforced the sealing of homes suspected to house victims of the disease. Individuals considered tainted through contact with the sick and who failed to follow isolation procedures were arrested and often condemned to death. In fact, contemporary iconography depicts public executions by firing squads or hanging from gallows erected in various city piazzas. In Monrovia, a crowd of desperate residents sought to break out of their prison by storming the barricades, hurling stones and attacking their jailers, only to be greeted with live ammunition firepower that managed to kill one boy and injure others. One dweller caught in the crossfire sarcastically asked ”you fight Ebola with arms?”
Risk fluctuates; it can be subjected to reevaluations within shifting social contexts and sanctioned by experts, then amplified by information systems for the purpose of mobilizing public opinion. This is particularly true if uncertainty, rumors, and a sensational media stoke fears of contagion, causing societal support systems like Monrovia’s public health departments and hospitals to break down. In the United States, three such intra-city quarantines were imposed in response to a pandemic of plague: Honolulu (1899-1900), San Francisco (March 1900) and again (May 1900). None proved beneficial.
Like Monrovia’s township, the targets were overcrowded and impoverished enclaves, unsanitary urban slums largely populated by Chinese migrants. In Hawaii, faced with a confirmed case of plague, the Honolulu Health Board issued an order to quarantine the Chinatown district on December 12, 1809 by roping it off with the help of rifle-toting National Hawaiian guardsmen. To avoid losses for white businesses, the perimeter was gerrymandered to exclude them. The afflicted neighborhoods, home to about 5,000 people--half of them Chinese--featured crumbling shanties with cesspools planted on stagnant marshy land strewn with refuse. In such circumstances, potentially plague-carrying rats posed an unacceptable risk.
Based on work by my colleague and friend James C. Mohr, frequent medical inspections and a search for new cases ensued. Disinfection, garbage removal, and the burning of “infected” lodging that had sheltered the sick began. The rationale for burning houses to kill plague germs stemmed from recommendations adopted by Hong Kong’s Sanitary Board during an epidemic in 1894 involving the walled-in and overcrowded and dilapidated district of Taipingsshan. While the official quarantine boundaries in Honolulu were constantly patrolled, security remained lax and direct contact with residents through the influx of food supplies and services continued. Yet, angry denizens protested the seclusion with threats, concealment, and flight. Businesses suffered, exports dwindled, and a paucity of new cases created pressures for the Health Board to terminate the quarantine six days after its initial decree. Reinstated on December 28 after the appearance of new cases, Honolulu’s quarantine was responsible for reducing Chinatown to ashes on January 20, 1900. With orders to burn down additional rat-infested housing, the local Fire Department misjudged the weather conditions: strong winds spread the flames to nearby buildings and a church, forcing residents to flee the district. The fire eventually scorched thirty three acres of the city and destroyed 40,000 homes. Rejected by dwellers from the outlying neighborhood, the Chinese were forced into makeshift detention camps, initially under monitored by national troops but soon replaced with Hawaiian Republic guardsmen. While the accidental fire and destruction of Honolulu’s Chinatown contributed to the eradication of plague, this episode remains a stark remainder of the adverse consequences of coerced mass segregation.

Honolulu Chinatown 1900 Quarantine
Given plague’s relentless march across the Pacific, and the close commercial ties with Honolulu, particularly the extensive sugar trade, San Franciscans braced for its arrival. Indeed, the events in Honolulu had already prompted an inspection of the city’s Chinatown by Health Board officials in early January 1900. The subsequent story is told in greater detail in my recent book Plague, Fear, and Politics in San Francisco’s Chinatown (2012). Not surprisingly, the death of a Chinese laborer on March 6 with a presumptive diagnosis of bubonic plague encouraged health officials to immediately impose a quarantine of the entire district. The enforcement was quite similar. Early Chinatown risers, including cooks, waiters, servants, and porters heading for their jobs outside the district, discovered that ropes encircled the space between Broadway and California, Kearny and Stockton Streets. Two policemen on every corner demanded that everybody turn around and return to their homes. Traffic was blocked and streetcars crossing through the area were not allowed to stop. Massive confusion ensued as frantic Chinese escaped across rooftops or sneaked through the lines, fearful that outside employers would dismiss them if they remained absent. In the confusion, stores closed although some provisions were passed across the lines. The quarantine hampered the movement of Western physicians living outside the district, preventing them from attending the sick at the Oriental Dispensary. Chinese passengers could not board river and coastal steamers to leave the city. Many managed to cross the Bay in small boats and find shelter in vegetable gardens of suburban friends and laundries. Others hid with Chinese cooks in private residences. Crowds quickly assembled in the streets, stunned by the encirclement. Rather than respond forcefully, the Chinese at first aimed for a restoration of harmony. For them the quarantine constituted an operation designed to impress the district’s ethnic population that the local health department and police were, after repeatedly faltering, up to their jobs.

San Francisco Chinatown 1900
Bacteriological confirmation of plague’s presence, however, remained elusive. Facing growing skepticism, the Health Board—like in Honolulu—unanimously voted to lift the “preventive” quarantine a few days later. No further cases of plague were found. The temporary encirclement of Chinatown, widely characterized by the press as “bubonic bluff,” turned into a setback for sanitarians: with regular scavenger service suspended, mountains of rotten food littered the streets, creating an unbearable stench while providing further food sources for its hungry rats. With the Honolulu experience vivid in their minds, Chinese residents expected another possible razing or burning of their homes. In a series of patterns replicated in the months ahead, laboratory findings and quarantine threats would be announced, manipulated, and denied in a climate of profound political and economic divisions. In the meantime, the reported mortality rate in Chinatown had dropped dramatically.
When cleaning and disinfection operations failed and an anti-plague vaccination program fizzled, San Francisco’s authorities decided to rent a number of grain warehouses at Mission Rock, a small island near the city’s port, converting the facilities into a temporary detention facility for Chinese suspected of suffering from plague. However, an empowered Chinese leadership hired prominent local lawyers and challenged the plan in federal court. Soon thereafter, in a landmark decision, the presiding judge ruled that all public health measures, while lawful, were not totally immune to judicial scrutiny. Inasmuch as they impaired personal liberties, totally arbitrary measures could not be permitted to stand. In this particular case, the quarantine was also racially discriminatory and harmful since confinement actually increased the risk of infection in the district.
Within hours, however, business leaders and health officials from San Francisco and California met to deal with a growing trade embargo against the state because of the presence of plague. The only proper response: reassure the trading world by sending a clear signal of California’s determination to control the presumed foe. Thus the Health Board was authorized to proceed immediately and once more close down Chinatown, again a “merely precautionary” move. Instead of ropes, a large police force and workmen descended on Chinatown, erecting a veritable fence around the district with wooden planks, posts, cement blocks, as well as barbed wire, creating an enclosure to seal off the entire area. The issue of detention centers for suspected plague victims raised, once more, its ugly head. To force the issue, San Francisco’s mayor refused to take responsibility for feeding the blockaded population.
By June 5, the Chinese leadership filed another judicial request in US District Court to stop the planned deportation. The federal judge immediately lifted the embargo on food supplies to Chinatown. He also delayed the removal of Chinese to the Mission Rock detention camp, but granted a continuance, further infuriating residents of the district. Many had already lost their jobs and were without food and other supplies. Because of growing shortages, prices for the remaining merchandise were skyrocketing. Thousands would soon be destitute and a serious disturbance was expected. While the case continued to be debated in court, protests and demonstrations escalated. Attorneys for the Chinese argued that by confining thousands of residents, the quarantine had, in effect, created a potential “plague quarter” capable of spreading disease to the rest of the city.
Ten days after the filing, the judge handed down his decision in favor of the Chinese plaintiffs. Like the previous ruling, the court employed the legal standards of due process and equal protection to grant the injunction against quarantine. Morrow ruled that the San Francisco Board of Health acted “with an evil eye and unequal hand” in an arbitrary and racially discriminatory manner, actually increasing rather than lowering the risks of infection in the isolated population. The siege of Chinatown was over. A defiant ethnic community with the help of the federal judicial system had managed to thwart two quarantines in the course of a few months. Municipal workers began taking down the makeshift fence that had encircled the district for sixteen days, allowing more than one thousand trapped Chinese residents to pour across the breached fences. Wagon after wagon of supplies arrived. After two weeks of fright, deprivation and protests, euphoria descended on Chinatown. Numerous celebrations marked the passing of the “fake” quarantine. During this judicial proceedings, only three additional deaths had been bacteriologically confirmed as caused by plague.
The above historical examples illustrate the challenges, hazards and futility of mass quarantines, their adverse economic impact and human toll. Public health is ill served when brutal coercion exacerbates mistrust and triggers hostility. Moreover, like in the Chinatown examples, forceful segregation was totally out of synch with the contemporary epidemiological understanding regarding disease transmission. In plague, the vectors were mostly fleas and rats instead of humans while Ebola fever is originally contracted from handling and cooking contaminated bush meat. Monrovia’s quarantine, imposed on an overcrowded population already burdened with poverty is unconscionable: the slum already shelters some ill and dying cases of the disease. Their contagious body fluids will only magnify the outbreak already in progress. As provisions dwindle in West Point, food prices will skyrocket, making them unaffordable and soon unavailable. Faced with a standoff, hunger and desperation will lead to further skirmishes with the military units guarding the township. Interviewed by a CNN reporter, one residents admitted: “The hunger, the Ebola, everything. I’m scared of everything!”
Sources:
Liberian News, August 17, 2014.
Margaret Chan, “Ebola Virus Disease in West Africa—No Early End to the Outlook,” New England Journal of Medicine.org, August 20, 2014.
Guenter B. Risse, “Pesthouses and Lazarettos,” in Mending Bodies, Healing Souls: A History of Hospitals, New York: Oxford University Press, 1999, pp. 190-216.
Alison Bashford and Claire Hooker, eds. Contagion: Historical and Cultural Studies, London: Routledge, 2001.
New York Times, August 21, 2014.
CBC News and CNN News, August 26, 2014.
Howard Markel, “The Concept of Quarantine,” in Quarantine!: East European Jewish Immigrants and the New York City Epidemics of 1892, Baltimore, Johns Hopkins University Press, 1997, pp. 1-12.
James C. Mohr, Plague and Fire: Battling Black Death and the 1900 Burning of Honolulu’s Chinatown, New York: Oxford University Press, 2005.
Guenter B. Risse, Plague, Fear, and Politics in San Francisco’s Chinatown, Baltimore: Johns Hopkins University Press, 2012.

